Histology Continued. Histology is the microscopic study of human tissue. We are going to be looking at and discussing different tissue types and layers on a microscopic level. Even if you don't understand it, I think you will at least find some of the pictures I have taken interesting.
Today's Medical Topic: Histology of Mammal Colon
*NOTE* Most of this will be based on assumptions of what is SUPPOSED to be there and my not actually be in this slide but I will do my best.
The Tissue Sample: Alrighty. Let's take a look.

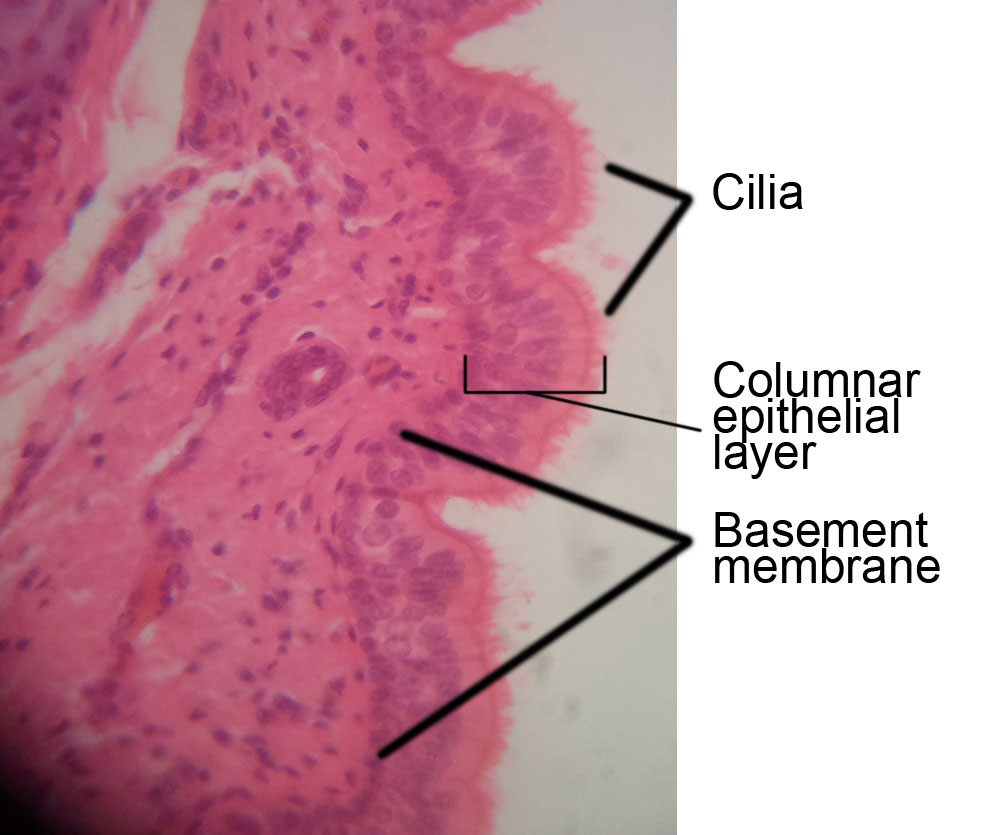
So from looking at other slides by people who are much smarter than I, I am assuming that layer at the top are goblet cells that secrete the mucus that lines your colon. If this is true then we can also assume that these goblet cells lay on a layer of sub mucosa. Which it is appears they do. As you know goblet cells are unicellular exocrine glands.
What is underneath the sub mucosa? I have no idea. Adipose? Some sort of loose connective tissue? Your guess is as good as mine.
That darker pink blob there is one of two things. It is either a piece of smooth muscle or a transverse section of a vein. I think it is a vein based on shape and size.
Let's get a little closer and see if we can figure something else out.

So I outlined a goblet cell in red. I am going with goblet cells on that part. There is the sub mucosa I mentioned earlier underneath the goblet cells. That other section. I got no fuckin idea. Maybe it didn't take up enough dye on this slide or it is old or something.
I am not willing to speculate any further about any other structures that are identifiable. You can look around and see if you can identify anything else yourself though. I hope you all enjoyed.


So from looking at other slides by people who are much smarter than I, I am assuming that layer at the top are goblet cells that secrete the mucus that lines your colon. If this is true then we can also assume that these goblet cells lay on a layer of sub mucosa. Which it is appears they do. As you know goblet cells are unicellular exocrine glands.
What is underneath the sub mucosa? I have no idea. Adipose? Some sort of loose connective tissue? Your guess is as good as mine.
That darker pink blob there is one of two things. It is either a piece of smooth muscle or a transverse section of a vein. I think it is a vein based on shape and size.
Let's get a little closer and see if we can figure something else out.

I am not willing to speculate any further about any other structures that are identifiable. You can look around and see if you can identify anything else yourself though. I hope you all enjoyed.
Send questions or comments to dudaday@gmail.com
Disclaimer: I am not a health care provider, any information presented in this blog should not be considered advice it is mearly an outlet to slake my curiosity. You should always consult your primary medical provider for any concerns or illness. Unlike Tylenol, I am not approved by the FDA or American Medical Association to treat or provide relief for any ailment.